Tube Feeding Patient and Family Resources
Tube feeding (enteral feeding) is a way of giving liquid nutrition (often formula) directly into the stomach or small bowel.
Tube feeding can be used for children or youth who:
- Cannot take food by mouth
- Have not learned to take food by mouth (oral aversion)
- Need extra nutrition
- Have problems swallowing
This is information about surgically placed feeding tubes.
There are many different types of feeding tubes and approaches to enteral feeding. The procedure and the type of feeding tube chosen for your child will depend on their healthcare needs. Tubes placed directly in the stomach are called gastrostomy tubes (GT). Tubes are sometimes placed in the small bowel (jejunum) when feeds are not tolerated via the stomach. These tubes are called jejunostomy or jejunal tubes (JT).
These are the different surgical procedures used to place feeding tubes at BC Children's Hospital:
- Percutaneous endoscopic gastrostomy (PEG)
- Open gastrostomy
- Laparoscopic gastrostomy
- Jejunostomy
- Gastrojejunal feeding tube (transgastric feeding tube)
- Open jejunostomy
- Roux-en-Y jejunostomy
- Braun jejunostomy
- Abdomen: contains the stomach, small and large intestines, liver, gall bladder, spleen, pancreas and bladder
- Aspiration: fluid in the lungs
- Abscess: a localized collection of pus in a tissue or body part resulting from the invasion of bacteria
- Decompression tube: a device which allows air/fluid to escape (venting) from the stomach via a feeding device
- Gastric decompression: removal of pressure in the stomach (usually through a nasogastric tube or gastrostomy tube)
- Gastric outlet obstruction: blockage at the end of the stomach
- Gastrostomy tube (GT): a feeding tube that supplies food directly into the stomach through a permanent surgical opening (gastrostomy) made into the stomach
- Gastrojejunal tube (GJ): a feeding tube (transgastric) that passes through the stomach through the gastrostomy into the jejunum
- Hypergranulation tissue (proud flesh): an overgrowth of fleshy tissue (granulation tissue) that often grows up around the tube
- Ileus: an intestinal obstruction either mechanical or functional
- Jejunal tube (JT): a feeding tube that supplies food directly into the small intestine (jejunostomy) made possible by a surgical opening into the small intestine or through a transgastric feeding tube into small intestine
- Jejunum: the second portion of the small intestine (small bowel)
- Laparoscopy: a surgical procedure that explores the abdomen using a type of endoscope (a camera) called a laparoscope
- Laparotomy: the surgical opening of the abdomen
- Nissen fundoplication: an operation used in treating stomach acid reflux into the esophagus. It is an operation where there is a 360 degree wrap of the greater curvature of the stomach around the intraabdominal esophagus
- Peristomal: area around the stoma
- Pyloroplasty: an operation where the pylorus muscle is partially divided to enlarge the outlet of the stomach and facilitate gastric emptying
- Reflux: backward flowing of a substance (e.g. return of fluids to the mouth from the stomach)
- Roux en Y jejunostomy: a surgical procedure that takes a portion of the jejunum and creates a limb that forms the stoma for the jejunostomy tube. This allows for a button or skin level device to be used as a feeding tube
- Stoma: an artificial opening
PEG
Image

A PEG feeding tube can last for 1-2 years. You can discuss changing to a lower profile feeding tube after 3 months. Most children are admitted for daycare surgery to have the PEG tube removed. The adapters (at the end of tube) sometimes leak - they can be easily changed (once a month). We recommend taping the tube to the abdomen to stabilize the tube.
MIC G (balloon-type device)
Image

MIC G tubes are sometimes used as primary (initial) tubes. They have a balloon. Subsequent tube changes can be done in the clinic or at home.
MIC KEY (balloon-type device)
Image

MIC KEYs are a balloon-type device as well. These tubes last anywhere from 3-6 months on average (depending on many factors). They are most often changed in the clinic or at home once families are comfortable with the process.
Nutriport (balloon-type device)
Image

Nutriports are a balloon-type device as well. These tubes last anywhere from 3-6 months on average (depending on many factors).They are most often changed in the clinic or at home once families are comfortable with the process.
Bard Button (mushroom-type device)
Image
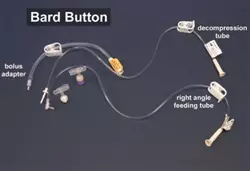
Bard buttons are a mushroom-type device that are most often changed in a clinic setting or operating room because we believe removing and replacing the device can be uncomfortable. Some children tolerate the tube changes in clinic without sedation, while others require medication to help them with the tube change.
Jejunostomy tubes
For Roux-En-Y or a Braun jejunostomies - the above low profile-type tubes may be used.
Image
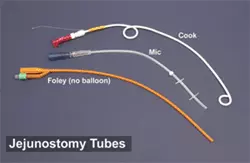
Here are three types of J tubes:
- Cook catheter - for transgastric jejunal feeding
- MIC - for a surgical jejunostomy
- Foley with no balloon - replacement tube for a surgical jejunostomy
There are several types of jejunostomy tubes used in our program. The type of tube used will depend on the way the jejunal feeding has been established. A lower profile device can be used to access Roux-En-Y jejunostomies and Braun jejunostomies.
Transgastric jejunal feeding tubes
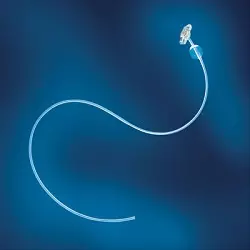
Cook catheter for transgastric jejunal (GJ) feeding
Image

The type of tube is inserted through an established gastrostomy tract in the radiology department. This tube needs to be well secured (taped) to the abdomen to prevent it from falling out. These tubes can be easily pulled out if not secured well. It is very important to make sure that medications are given separately and flushed well to prevent the tube from becoming blocked. We often suggest that the tube is changed every 3 months on a routine basis.
MIC low profile transgastric jejunal feeding tube with gastric port
Photo to come.
MIC low profile transgastric jejunal feeding tube without gastric port
Image
MIC transgastric jejunal feeding tube
Image

A GJ tube is a radiologically inserted tube that is placed through the already established gastrostomy stoma and threaded into the jejunum in the x-ray department.
GJ tubes are used for children who cannot tolerate feeding into the stomach, usually due to gastroesophageal reflux (GERD).
To change a GJ tube in radiology:
- A requisition must be sent to the x-ray department for every tube change
- A doctor with admitting privileges at BC Children’s Hospital must sign the requisition
- GJ feeding tubes are routinely replaced on Thursdays
Important things to know about a GJ tube
- Feeding will now need to be continuous. The small bowel cannot handle bolus feeds like the stomach can. You will no longer be able to bolus feed with this type of feeding tube
- The length of feeding time will increase if you have been bolus feeding
- The GJ tube may not be as secure as the GT. It can fall out if it is not taped and secured well (if a Cook catheter is used)
- The GJ tube tends to block easier that the GT. Flush the tube well before and after medications
Preventing the tube from falling out
If you are using a Cook catheter, you need to keep the GJ tube well secured. There is no balloon or disc that keeps the tube in the small bowel.
- Keep tube well secured to the abdomen with waterproof tape
- A piece of duoderm on the skin may help to protect the skin. The tape needs to be changed frequently
- Always carry a replacement tube with you
- Place the replacement tube into the stoma to stop the stoma from closing
- You can purchase an emergency kit at the outpatient pharmacy in the Ambulatory Care Building
If the tube falls out
If the GJ tube falls out, a replacement tube needs to be placed into the stoma as soon as possible so that the hole does not close over. You can use a Foley catheter to keep the stoma open until the GJ tube can be replaced.
- If your child can tolerate medications and fluids via the gastrostomy, you can use this route until the tube is replaced
- If your child can NOT tolerate any fluid via the gastrostomy, you need to take your child to a hospital for intravenous fluid until an appointment can be arranged to replace the GJ feeding tube
Do not panic
If the stoma is new (the gastrostomy tube was inserted less than six weeks ago):
- Cover the stoma with a clean gauze or cloth
- See a doctor to put the tube back in as soon as possible (within two hours)
- The stoma will close quickly (within four to six hours)
If the stoma is more than six weeks old:
- Place a feeding tube into the stoma as soon as possible
- Gather equipment:
- Feeding tube (Foley catheter or skin level tube)
- Wash cloth
- Tape
- 5ml syringe – to inflate the balloon
- 5ml water – to inflate the balloon
- Water-soluble lubricant (like KY jelly)
- Draw up 5ml of water into the syringe
- Check the balloon on the new tube before putting it into the stoma by inflating the balloon with 5ml of water
- Deflate the balloon by pulling the water back into the syringe
- Moisten the end of the tube with water or water-soluble lubricant (to make the tube go in easier)
- Insert the new tube about 2 inches into the stoma. Inflate the balloon with the 5 ml of water in the syringe. Remove the empty syringe from the tube
- Gently pull back on the tube, to feel the balloon snug against the stomach wall
- Arrange to have the GJ tube replaced
- Your doctor will have to arrange to have the tube changed
- If your child can not have medications and/or fluids via the gastrostomy route, you will need to go to the hospital for intravenous fluid until an appointment can be booked to have your tube changed
- Gather equipment:
If the GJ tube becomes blocked
First try using warm water and use a firm push/pull action with a 60ml syringe to unblock the tube. If this is not successful, use a mixture of cotazym and sodium bicarbonate to unblock the tube. Your doctor will need to supply you with a prescription for the cotazym capsules.
Supplies
- Doctor must prescribe a cotazym capsule (pancreatic enzyme)
- Cotazym capsules are available at a pharmacy
- Sodium bicarbonate 1 tablet (325mg) or ½ teaspoon of baking soda
- Warm water
- Syringe (60ml)
- Small cup
Method
- Try to unblock tube with warm water using a firm push/pull action
- Pull out as much of the contents of the tube as you can
- Place contents of cotazym capsule (just the powder) and crush sodium bicarb tablet (baking soda) into cup
- Add 10-15ml of warm water to the powders and mix very well
- Draw up this solution into the syringe (60ml)
- Put the solution into the blocked tube and let it sit for 15-30 min
- You can “milk” the tubing to move the solution through the tube
- Flush the tube with warm water using the push/pull action
- If tube is still blocked, repeat above. You may leave the solution in place for one (1) hour
- If two (2) attempts to unclog the tube do not work – contact your doctor or remove the tube and use as a gastrostomy until the GJ tube can be replaced
Problem: blocked tube
Prevention is the key. Flush, flush, flush.
Possible causes:
- Feeds too thick
- Residue build up in the tube
- Medicine too thick (some medicines can block the tube)
Action
- Flush tube with warm water before and after feeds and medications
- Ensure that blender-prepared foods are in liquid form
- Crush tablets to a fine powder and dissolve in a small amount of warm water
- Do not give enteric-coated and time-release medication through the tube
- If tube is blocked, may need to order for cotazym and bicarb to unblock tube
- Do not mix medications together
Problem: irritation around tube site (stoma)
- Sucralfate/DESITIN (3% in 25 grams) for "burned" skin
- Cicatrin powder for wet and mucky skin
- Proshield as a protective barrier if required
Possible causes:
- Tube movement
- Tension on the tube
- Leaking from around the tube
Action:
- Ensure that tube is secured to decrease movement
- Gently pull up on tube to ensure balloon/end of tube is up against the stomach wall
- Be aware of marking of tube at abdomen (if it is not a low profile tube)
- Assess patency of balloon, ensuring that water in balloon is intact for established tracts (more than 6 weeks old)
Problem: migration of the tube
Possible causes:
- Internal migration tube sliding further into the stomach
- External migration tube sliding out and sticking to the stomach wall
- Intraperitoneal tube - out of the stomach - between stomach and skin
Action:
- Observe for signs of obstruction: vomiting, epigastric pain, increased leakage around the tube
- Stop feeds immediately if migration to peritoneal cavity presumed
- Call doctor if: pain, abdominal distension, nausea, vomiting, fever, swelling around the tube site and pain on feeding or flushing
Problem: granulation tissue (hypergranulation tissue) – proud flesh around the tube site
Possible causes:
- Body "walling off" from the tube
- Body's reaction to the tube
Action:
- May cauterize with silver nitrate sticks or treat with a short term low dose cortisone cream
- Consult surgical nurse or physician
- Ensure that tube is stable
Problem: choking or coughing during feed
Possible causes:
- Tube in the wrong place
- Gastroesophageal reflux
Action:
- Elevate head for feedings
- Notify physician if continues
Problem: constipation
Possible causes:
- Low stool volume
- Lack of bulk in diet
- Inadequate fluid intake
- Medications
Action:
- Consult physician and/or dietitian
- Encourage activity
- Increase water intake
Problem: vomiting
Possible causes:
- Too rapid infusion of feed
- Excessive amount of feed
Action:
- Reduce rate of feed
- If vomiting continues, stop feed and reassess rate, type and consult a physician or dietitian
Problem: diarrhea
Possible causes:
- Feed infusing too quickly
- Feed too cold
- Contamination of food or feeding equipment
- Lack of bulk in diet
- High osmolality of formula
Action:
- Reduce rate of feed
- Infuse feed at room temperature
- Check proper handling of equipment
- Consult dietician for dietary changes or rate and concentration of formula
Problem: psychosocial and emotional concerns
Possible causes:
- Feelings of dependency, loss of control, loss of social aspect of eating, feelings of being different and change in body image
Action:
- Preoperative session for information exchange
- Set goals
- Adjust feeding schedule around activities and schooling
- Plan feeding around meal times
- Include the enterally fed child with family meals
Supplies and methods
Using pancreatic enzymes
Supplies
- Doctor must prescribe a cotazym capsule (pancreatic enzyme)
- Cotazym capsules are available at a pharmacy
- Sodium bicarbonate 1 tablet (325mg) or ½ teaspoon of baking soda
- Warm water
- Syringe (60ml)
- Small cup
Method
- Try to unblock tube with warm water using a firm push/pull action
- Pull out as much of the contents of the tube as you can
- Place contents of cotazym capsule (just the powder) & crush sodium bicarb tablet (baking soda) into cup
- Add 10-15ml of warm water to the powders and mix very well
- Draw up this solution into the syringe (60ml)
- Put the solution into the blocked tube and let it sit for 15-30 min
- You can “milk” the tubing to move the solution through the tube
- Flush the tube with warm water using the push/pull action
- If tube is still blocked – repeat above. You may leave the solution in place for one (1) hour
- If two (2) attempts to unclog the tube do not work – contact your doctor
Do not panic
If the stoma is new (the tube has been in for less than six weeks)
- Cover the stoma with a clean gauze or cloth
- You need to have a doctor put the tube back in as soon as possible (within two hours)
- The stoma will close pretty quickly (we usually say four to six hours)
- Often we will take an X-ray with contrast (dye) to make sure the tube is in the right place before we can re-start feeds
If the stoma is more than six weeks old
- You need to place a feeding tube into the stoma as soon as possible
- PEGs and Bard buttons cannot be replaced. You will have to use the Foley catheter from your emergency kit
- You can re-insert MIC KEYs and MIC Gs
- Always make sure you get contents returned before restarting feeds
Remember to always carry a replacement tube with you.
- You will need to place the tube into the stoma to stop the tract/hole from closing.
Steps to reinserting the gastrostomy tube
- Image

Gather equipment
- Feeding tube (Foley catheter or skin level tube)
- Wash cloth
- Tape
- 5ml syringe – to inflate the balloon
- 5ml water – to inflate the balloon
- Water soluble lubricant (like KY jelly)
- Draw up 5ml of water into the syringe
- Check the balloon on the new tube before putting it into the stoma by inflating the balloon with 5ml of water
- Deflate the balloon by pulling the water back into the syringe
- Moisten the end of the tube with water or water-soluble lubricant (to make the tube go in easier)
- Insert the new tube about two inches into the stoma
- Inflate balloon with the 5 ml of water in the syringe – remove the empty syringe from the tube
Gently pull back on the tube – to feel it snug against the stomach wall.
Clean and dry the skin – tape the tube to the skin to secure.
If using a catheter you should mark where the tube comes out of the body – you can use this as a “check-mark” for placement.
Check the placement of the tube by withdrawing stomach contents – make sure this fluid goes back into the stomach.
If unable to withdraw stomach contents – reposition and try again. If you can not get any stomach contents – wait ½ hour and try again. If unsure that the tube is in the stomach – do not use the tube.
Do not panic
Remember to always carry a replacement tube with you.
If the stoma is new (the tube has been in for less than six weeks):
- Cover the stoma with a clean gauze or cloth
- You need to have a doctor put the tube back in as soon as possible (within two hours)
- The stoma will close pretty quickly (we usually say four to six hours)
If the stoma is more than six weeks old:
- You need to place a feeding tube into the stoma as soon as possible
- You will have to use the Foley catheter from your emergency kit to keep the stoma/hole open until a new GJ tube can be reinserted
Steps to reinserting a gastrostomy tube
Even if your child/youth does not tolerate feeds via the stomach, you still need to place the tube to keep the stoma open.
- Image
Gather equipment:
- Feeding tube (Foley catheter or skin level tube)
- Wash cloth
- Tape
- 5ml syringe – to inflate the balloon
- 5ml water – to inflate the balloon
- Water
- Soluble lubricant (like KY jelly)
- Draw up 5ml of water into the syringe
- Check the balloon on the new tube before putting it into the stoma by inflating the balloon with 5ml of water
- Deflate the balloon by pulling the water back into the syringe
- Moisten the end of the tube with water or water-soluble lubricant (to make the tube go in easier)
- Insert the new tube about two inches into the stoma
- Inflate balloon with the 5ml of water in the syringe – remove the empty syringe from the tube
- Gently pull back on the tube – to feel it snug against the stomach wall
- Clean and dry the skin – tape the tube to the skin to secure
- You will need to arrange to have the GJ tube replaced
If your child cannot have medications and/or fluids via the stomach (GT), you will need to go to the hospital for intravenous fluid until an appointment can be booked to have your tube changed.
Your primary health-care physician will need to arrange to have the GJ tube replaced in the Xray department.
Your doctor or nurse will discuss how to replace and manage this tube with you as there are so many different ways to place a jejunostomy tube.
Roux-en-Y
If the stoma is new (the tube has been in for less than six weeks)
- Cover the stoma with a clean gauze or cloth
- You need to see a doctor to put the tube back in as soon as possible (within two hours)
- The stoma will close pretty quickly (we usually say four to six hours)
If the stoma is more than six weeks old
- You need to place a feeding tube into the stoma as soon as possible
- The Foley catheter of a MIC KEY – remember to use only 2-3ml of water to inflate balloon
Braun jejunostomy
We usually replace Braun-type jejunostomy tubes in clinic as they can be a little more difficult to place.
If you have been instructed to replace the tube
- Image
Gather equipment: feeding
- Draw up 2-3ml of water into the syringe
- Check the balloon on the new tube before putting it into the stoma by inflating the balloon with 5ml of water
- Deflate the balloon by pulling the water back into the syringe
- Moisten the end of the tube with water or water-soluble lubricant (to make the tube go in easier)
- Insert the new tube about two inches into the stoma
- Inflate balloon with the 2-3ml of water in the syringe – remove the empty syringe from the tube
- Gently pull back on the tube
- Clean and dry the skin
Hypergranulation tissue is believed to occur as a result of an extended inflammatory response. We believe it may be caused by a reaction to the tube - the body is in fact "walling off" the tube.
Pressure, moisture and friction may also contribute to the development of hypergranulation tissue. Hypergranulation tissue is the body’s way to fight the gastrostomy tube. The body does not think the tube belongs there.
Image

- Hypergranulation tissue is not harmful
- Hypergranulation tissue is red, moist and bleeds when rubbed
- Hypergranulation tissue oozes a yellow, sticky drainage
- Hypergranulation tissue can affect how the gastrostomy or jejunostomy tube fits in the stoma
- Hypergranulation tissue is common in the first 3 months
If granulation tissue occurs
Image

Call your nurse of doctor to ask about silver nitrate sticks. They help to remove the hypergranulation tissue. Currently we recommend that the site be kept as clean and dry as possible. We treat the tissue with either silver nitrate sticks or a low dose cortisone cream (Triacet 0.1%) for 5-7 days.
Silver nitrate application
Take the following steps once a day for five days:
- Put a layer of petroleum jelly (Vaseline) on the healthy skin around the granulation tissue before using the silver nitrate stick – the silver nitrate will injure the healthy skin
- Moisten the tip of the silver nitrate stick with water
- Touch the silver nitrate stick onto the granulation tissue – red, raised skin
- Protect clothing from being stained by the silver nitrate (will turn black) by putting a small gauze square over the area and taping it
- If there is no improvement in five to seven days, call the nurse or doctor
There are several ways that we can place (insert) a feeding tube for an individual. The surgeon will choose the procedure that is most appropriate for each individual child and their health-care situation.
PEG tube
- Image
This is a percutaneous endoscopic gastrostomy. The child is given an anesthetic or is sedated during the procedure
- An endoscope is passed down the child’s throat and all the way into the stomach
- The doctor makes an incision (stoma) into the stomach. They insert a thread into the stoma, then pull it back through the child’s throat and out the mouth
- They tie the feeding tube (PEG tube) onto the thread and pull it out through the opening in the stomach wall (stoma)
- The tube has a disc that prevents the tube from pulling all the way out of the stoma
- They attach a bumper or disc is attach to the tube from outside the body, to help stabilize the tube and work with the internal disc to keep the stomach wall tight against the abdomen
- Most often the tube can be used for feeding the same day
- Healing is quick. There is one small incision
- We cannot perform the PEG method on all children
Surgical gastrostomy (open) tube
- A child may need a surgical gastrostomy if we cannot easily pass a scope to the stomach; the abdomen is already surgically opened for another procedure; or the position of the bowel will impede inserting the tube through the PEG route
- When using the surgical method, we make two incisions (cuts)
- The surgeon puts a tube with a balloon or mushroom-shaped bulb at one end into the stomach through the larger incision
- They pull the other end through the second small incision (stoma) and secure the tube
- They then stitch the stomach to the abdominal wall
- The bulb/balloon helps prevent the tube from falling out
- Examples of tubes that may be used in a surgical gastrostomy include Foley catheters, Malecot catheters, Bard buttons, MIC KEY buttons and MIC G tubes
Laparoscopic gastrostomy tube
- This is a minimally invasive approach to inserting a gastrostomy tube using an endoscope called a laparoscope
- Often we place a skin-level device or a MIC G tube as the primary tube
- There will be two small incisions at the umbilicus (belly button)
Jejunostomy tube (JT)
There are several ways to create a jejunostomy feeding tube:
Open jejunostomy
- This surgical method requires two abdominal incisions. We make them a small distance apart
- The surgeon creates an opening into the jejunum through the first and larger incision
- They place a feeding tube into the jejunum and pull the tube through the other incision. We use a MIC jejunostomy tube or a Foley to access this site (as a feeding tube)
- They stitch the jejunum against the abdominal wall and close the larger incision
- The may put in a stitch to secure the tube to the skin, to hold the tube in place during the healing phase
Roux-en-Y
- This is another type of jejunostomy
- The surgeon takes a portion of the jejunum and creates a short blind-ending limb into which they insert the jejunal tube
- There is one incision, and a separate opening for the JT (usually a MIC G)
- We may insert a skin-level device after three months
Braun-type jejunostomy
- This is another type of jejunostomy
Transgastric feeding tube (GJ)
- This is a feeding tube that goes into the jejunum (small bowel) through an already established (more than 6 weeks) gastrostomy
- We guide the tube into place with the help of x-ray type images that show up on a special screen
- The radiology department inserts the tube. We arrange insertion/reinsertion through the radiology department
Activity
- Wait at least five days after surgery before swimming or bathing. If you have a PEG tube, ensure the tube is securely taped to the abdomen with waterproof tape
- Children can lie in any position they find comfortable including their stomach. You can cover the tube up with clothes to try and keep the child from pulling or playing with it
- Children can participate in sports once the new site is no longer tender. For PEG tubes, ensure you have taped them securely to the abdomen. If there is a blow to the abdomen, there may be some pain. It is not an emergency unless there is severe pain, persistent pain that does not improve, bleeding, or bruising. If this occurs, then contact your doctor
Care of the stoma site
Goal: keep the site as clean and dry as possible.
- Do not routinely turn the new tube for 6 weeks following surgical placement
- Do not deflate the balloon on a new tube for at least 6 weeks after surgical placement
- Always wash your hands before caring for the stoma or feeding tube. Hand-washing is one of the best ways you can prevent the spread of illness
- Clean the area around the tube at least twice a day and inspect surrounding skin for any signs of redness, irritation or infection
- Clean around the tube with a clean wash cloth, cotton balls or Q-tips and some warm, mildly soapy water. Rinse and dry the area well
- Gently clean under the disk or around the tube, the outside of the tube, and the skin surrounding the tube with warm soapy water. Rinse it with warm water and then gently pat it dry or let it air-dry
- Exposure to air is an excellent way to heal skin and to keep it in healthy condition
- When securing the tube with tape, rotate the position of the tape so it does not cover the same piece of skin each time. This will help to maintain healthy skin and decrease irritation
Care of the feeding tube itself
- Inspect the feeding tube for cracks and or leaks
- For PEG, MIC G and Foley tubes - know the correct length of your child’s feeding tube. Measure the length of the tube that is on the outside of the body. If it is shorter than usual, gently pull on it until it is the appropriate length. If it is longer than usual, do not use the feeding tube and call your doctor. Knowing the correct length of the feeding tube helps ensure that the tube is in the correct position in the body for safe feeding
- You may need to measure low-profile tubes if your child gains weight or their abdominal girth changes. We can measure tubes to ensure they fit correctly
Care of equipment
This is important to prevent bacteria from growing.
- After every feeding, wash the equipment (feeding bag, tubing, etc.) with hot soapy water. Use a bottle brush if necessary to ensure you remove all formula from the bag. Rinse well with hot water. Make sure to remove excess water from the feeding set and adapters
- Between feeds, wrap the equipment in a clean towel and store it in the refrigerator. The cool temperature helps decrease the growth of bacteria
- Once a day you need to take the syringes apart, wash them with hot soapy water, rinse them and let them air-dry
- After the last feeding of the day, wash the bag and tubing as usual with hot soapy water and then rinse with a vinegar solution (1/4 cup vinegar to 1 cup water). Rinse again with hot water and store as usual in the refrigerator
- Change feeding bags and syringes about twice a week, or earlier if necessary
- Change adapters and connectors every two to four weeks (sometimes more often if feeds are continuous)
Tube feeding tips
- If the tube feeding bag is starting to smell sour or starts changing to a different colour, throw it away
- Allow formula to warm up to room temperature before using. Cold formula can cause cramping
- Do not microwave the formula, as this can cause the proteins in the formula to break down
- Throw out open containers of formula if not used within 24 hours, even if they were refrigerated
- Throw out any formula that has been left at room temperature for more than four hours
- Remember that hand washing is key in preventing the spread of bacteria
Mouth care
Important for maintaining the normal conditions of the mouth when children cannot have foods orally.
Steps you can take to ensure proper mouth care:
- Rinse your child’s mouth out four to six times a day with water, mouthwash, a cloth, or Toothette.
It is important to make sure your child’s teeth are brushed twice a day - Keep lips moist
- At the advice of a doctor, children can suck candies, soothers, etc. to help with the flow of saliva (oral stimulation)
Oral stimulation
- This gives the child sensory experiences in and around the mouth and encourages them to use their lips, jaw and tongue
- We use oral stimulation in children who cannot take food by mouth, because they rarely use (or stimulate) their mouth. It can develop a hypersensitivity to touch which makes the possible return to oral foods much more difficult
- Through stimulating the mouth with touch, tastes and different temperatures of food, we can sometimes prevent hypersensitivity
Oral stimulation is important because it:
- Allows a child to develop and maintain movement patterns for eating and swallowing
- Prevents hypersensitivity
- Allows the child to experience pleasures associated with tastes, textures, smell, touch and social time surrounding eating
To promote oral stimulation:
- Before feedings, use a wash cloth and gently wash the face. Wash the cheeks and forehead first and slowly move towards the mouth. If the child shows distress, stop and try again the next day
- You can use a soother, toothbrush, or the child’s hand in the mouth
- Associate meal time and eating with pleasure
- Consult your physician or occupational therapist for additional ideas and advice on what your child can have in their mouth
- A gastrostomy is a way to feed directly into the stomach and a jejunostomy feeds directly into the small bowel (intestine)
- You cannot bolus feed through a jejunostomy tube. The diameter of the small bowel will not tolerate the volume the way the stomach does
How to prevent the feeding tube from becoming blocked
- Flush, flush, flush
- Flush with water after each feed and after each medication
- Do not mix medications in the same syringe
- Try to use a liquid form of medication if available
- Avoid using the antibiotic clarithromycin
What to do when the feeding tube is blocked
- Try to flush with warm water using a push/pull method to try to unplug the tube
- If this is unsuccessful, try using a cotazym capsule mixed with sodium bicarbonate and water to unplug the tube
- Mix the powder of a cotazym capsule with 1/2tsp of baking soda or 325mg of sodium bicarbonate with a some warm water
- Put this mixture into the feeding tube
- Use the push/pull method to try to unblock the tube
- You can repeat this two (2) times
- You can leave the solution inside the tube for up to one (1) hour
- If this is unsuccessful, you will need to arrange to have the feeding tube changed
Hypergranulation tissue
- Hypergranulation tissue is believed to occur as a result of an extended inflammatory response
- We believe it may be caused by a reaction to the tube. The body is in fact "walling off" the tube
- Pressure, moisture and friction may also contribute to the development of hypergranulation tissue
- Hypergranulation tissue leaks a yellow, sticky drainage. People often describe it as itchy. This tissue may bleed easily
What to do with hypergranulation tissue
Hypergranulation tissue (proud flesh) can affect the seal of the feeding tube. It may increase the amount of stomach contents that leak from the stoma. The drainage from the tissue can irritate the surrounding skin.
Silver nitrate application
You can use silver nitrate sticks to cauterize (burn) the hypergranulation tissue. We suggest a five-day course of once-a-day treatments. Ensure that the surrounding skin is well protected prior to treating the hypergranulation tissue.
Cortisone cream application
You can also apply a short course of a low-dose cortisone cream to the hypergranulation tissue as ordered by a health care provider.
What to do if the feeding tube falls out
- Do not panic – this is not an emergency
- When a feeding tube falls out, the stoma will start to close. Some stomas can close in a few hours
- Always carry your emergency replacement kit which should include:
- Replacement feeding tube (Foley/replacement tube)
- 5 ml syringe
- Water
- Clamp or cap (for Foley)
- Washcloth
- Water-based lubricant
- Waterproof marker
- Emergency phone numbers
- Change for a phone call
- Notes on replacing the GT
- If the gastrostomy is new (the operation/procedure was in the last six weeks), a doctor should reinsert the tube (to make sure that the feeding tube goes back into the right spot), unless your doctor directs otherwise
- Otherwise you need to:
- Wash your hands
- Draw up 5ml water into your 5ml syringe
- Have child lying flat – relaxed if possible
- Fill the balloon with water, to check the balloon for leaks
- Remove the water from the balloon
- Put lubricant on the end of the tube
- Put the moist tube into the stoma. Hold the end of the tube upright so it won’t leak on you
- Use the syringe to put 5ml of water into the balloon port, then remove the syringe
- If you feel resistance, don’t use force. Try again
- Pull gently on the tube to ensure that the balloon is snug against the stomach wall
- Close the tube and clean the skin around the tube well
- Mark the tube (if using a Foley) at skin level with a waterproof marker
- Secure the tube in place with tape
- If you are not sure that the feeding tube is in the right place – DO NOT use the tube for feeding. Contact your doctor
When to call the surgeon, and which doctor to call for concerns about your child's feeding tube
- Most children who are on home-feeding regimes are under the care of a pediatrician. Your pediatrician or family doctor will follow your child’s feeding and weight gain concerns
- Map out a plan of who is available in your community. You can discuss this with your health-care provider
- Call your child’s surgeon if there is a fever, redness, swelling or green drainage from the stoma site around the time of surgical insertion (first 3 months)